[Association of American Medical Colleges\COVID-19]
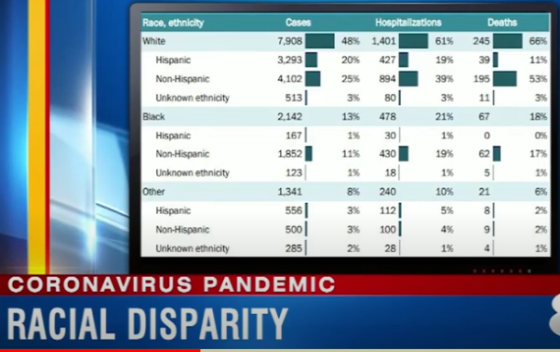
Dr. David Acosta: “Local data – from Connecticut to Michigan, from New York to Louisiana – are telling the same story: people of color, particularly Black Americans, are more likely to get sick and die from the novel coronavirus.”
Photo: YouTube
The Association of American Medical Colleges (AAMC) is calling for a COVID-19 data collection system to better understand racial disparities.
With the coronavirus (COVID-19) pandemic illuminating longstanding social, economic, and health inequities in the United States and around the world, the Association of American Medical Colleges today called for the development of a national, standardized data collection system.
This system would accurately capture race and ethnicity data, as well as information on the social and environmental conditions in which people live, work, and play (e.g. crowding, access to food, housing security, etc.) that impact how illness can spread.
The AAMC also recommended capturing community-level data that adequately reflect the neighborhoods to which COVID-19 patients are discharged, noting that county or zip code data are not specific enough for densely populated communities likely to be most impacted by infectious disease. Engaging state and local public health departments, private testing labs, and hospitals – all at the front lines of the pandemic response – in the data collection effort is also essential to avoid undue burden on these systems.
“Local data – from Connecticut to Michigan, from New York to Louisiana – are telling the same story: people of color, particularly Black Americans, are more likely to get sick and die from the novel coronavirus,” according to David A. Acosta, MD, AAMC chief diversity and inclusion officer. “This is not because the virus is naturally more harmful to racial and ethnic minorities. Rather, this is the result of policies that have shifted opportunities for wealth and health to a narrow segment of society. Black, Hispanic, and Native Americans, the poor, the homeless, immigrants, and people who are incarcerated find themselves with fewer economic resources and with physical health conditions that make them and their communities more vulnerable to illnesses like COVID-19.”
“These disturbing data demonstrate the stark health disparities in our nation, including higher rates of diabetes, asthma, and hypertension, and historical events that have disproportionally impacted communities of color and caused long-term problems and increased mortality rates,” continued Acosta. “Better data on the current pandemic will give us an opportunity to take decisive action to protect vulnerable communities and prevent further catastrophic outcomes.”
“While health inequities related to COVID-19 are most certainly developing in real-time, the fact is that our current data collection efforts are inadequate and do not give us a complete picture,” said Ross McKinney, MD, AAMC chief scientific officer. McKinney noted that the continued scarcity of tests and the message to stay home if symptoms are mild or moderate during this pandemic has resulted in many people with COVID-19 who have not been tested for the coronavirus and therefore are absent from local and state data.
“Additionally, a city-by-city variation of who gets tested – either due to CDC guidance, local policies, or community mistrust of government institutions – could be causing certain groups to remain untested, leaving the data biased and potentially misleading,” said McKinney. “Finally, current local data reports have noted a significant amount of ‘missing data,’ meaning data about race or ethnicity were not captured and reported.”
To address these shortcomings and to more effectively mitigate health inequities going forward, the AAMC recommends that future data collection efforts and surveillance be patient-centered and developed in collaboration with local community members and community-based organizations who have trusted and established relationships with local residents and leaders. Collecting valid data that both identifies communities disproportionally at-risk and suggests structural interventions is crucial to ensuring just, equitable preparedness and response during a pandemic.
To access the AAMC’s coronavirus resources for the academic medicine community, visit www.aamc.org/coronavirus.
The AAMC (Association of American Medical Colleges) is a not-for-profit association dedicated to transforming health care through innovative medical education, cutting-edge patient care, and groundbreaking medical research. Its members are all 155 accredited U.S. and 17 accredited Canadian medical schools; nearly 400 major teaching hospitals and health systems, including 51 Department of Veterans Affairs medical centers; and more than 80 academic societies. Through these institutions and organizations, the AAMC serves the leaders of America’s medical schools and teaching hospitals and their more than 173,000 full-time faculty members, 89,000 medical students, 129,000 resident physicians, and more than 60,000 graduate students and postdoctoral researchers in the biomedical sciences. Additional information about the AAMC and its member medical schools and teaching hospitals is available at www.aamc.org.







